Married couple, Michael and Lila R., are longtime patients of Park Sports Physical Therapy. Michael is a lifelong athlete having run 26 marathons during his lifetime. He has also been a member of the Prospect Park Track Club, a local running club in Park Slope, Brooklyn. Michael has over 30 years of running under his belt. That’s a whole lot of miles!
His wife Lila, also an athlete, has spent most of her life swimming and running.
Lila’s first experience at Park Sports started back in 2011. She came in with a rotator cuff condition. One of our therapists treated her and got her back to swimming fairly quickly. Lila recommended her husband, Michael also get treated at Park Sports after her positive experience.
Michael suffered from arthritis in both his knees. It was when he tripped and injured his iliotibial band that he came in for treatment. He was feeling a snapping sensation whenever he would walk up and down stairs.
Kristin Romeo, DPT became both Michael’s and Lila’s therapist, often times seeing them at the same time for treatment. For Michael, Kristin used manual therapy, stretching, strengthening exercises, and worked on improving his balance on the injured leg.
During the interview, Michael and Lila spoke very highly of Kristin, saying “Kristin is attentive, listens to your needs, and makes sure that the problem area is getting the right treatment.”
“The sessions hold me accountable,” Michael mentioned. The exercises have helped him greatly throughout his treatment. He’s progressed to the point where he no longer feels any snapping sensation walking down the stairs.
Lila similarly was very pleased with her progress.
Michael and Lila, being older in age, both realize the importance of maintaining balance to avoid falls. Physical therapy has proven to be quite useful in that regard.
Both Michael and Lila recommend the services at Park Sports highly saying, “almost all our friends in the neighborhood go to Park Sports for physical therapy. This is a great place that offers excellent care. The therapists that work here are excellent. We couldn’t be happier with Kristin’s care.”
Injuries to the shoulder are fairly common in everyday life. Strains and sprains resulting from repetitive activities such as throwing a ball or twisting your arm while reaching behind your car seat happen all the time, and usually heal on their own in only a few days. But what happens if your shoulder suddenly starts to lose its normal range of motion for an unexplained reason?
In this article, I would like to talk about the diagnosis known as adhesive capsulitis, more commonly referred to as frozen shoulder.
What is Frozen Shoulder?
Frozen shoulder is a fairly common diagnosis, but is not well understood and does not always have a known cause. Many people develop frozen shoulder following a surgical procedure to the shoulder, or after an injury that results in the shoulder needing to be immobilized for a short period of time. However, in some cases, some people develop symptoms with no known trigger.
The symptoms are fairly clear-cut – a marked loss of normal range of motion and stiffness of the shoulder joint that may or may not be accompanied by pain.
This shoulder stiffness affects motion in all directions such as reaching up in the air or trying to place the hand behind the back or behind the head. Adhesive capsulitis begins as an inflammatory process within the shoulder and leads to scar tissue formation which can restrict shoulder motion.
For some people, this scar tissue formation can lead to pain in the shoulder joint, especially with movement and during the evening hours while trying to sleep.
The Stages of Frozen Shoulder
Physical Therapist, Edward Umheiser, DPT treating a patient with frozen shoulder.
There are several stages of frozen shoulder each with their own unique characteristics:
Inflammatory Stage
The inflammatory stage lasts approximately three months and is characterized by pain with shoulder movement in most directions. Pain is often sharp with movement at the end of the range, and there is an ache at rest. Pain is also commonly felt at night, making it difficult to fall asleep. The range of motion may still be normal at this early stage.
Freezing Stage
Edward Umheiser, DPT measures the shoulder’s range of motion.
The freezing stage typically lasts 3-9 months. This is when flexibility of the shoulder begins to reduce due to pain. At this time, people often begin to notice difficulty reaching overhead, or reaching behind their back. This stage, known as the frozen stage, is when the stiffness is most severe. The inflammatory process inside the shoulder joint is starting to decrease at this stage so pain is lessened or non-existent. Over the past several months a thick layer of scar tissue has formed around the shoulder capsule, which makes it difficult to move. This is the stage when most people are diagnosed with frozen shoulder.
Thawing Stage
Edward Umheiser, DPT treating a patient with frozen shoulder. With consistent physical therapy sessions, a patient can begin seeing an increased range of motion.
Finally, the thawing stage is when shoulder motion gradually starts to return to normal. This stage can last anywhere from 9 months to two years and may leave some minor limitations in shoulder range of motion afterward.
Treating A Frozen Shoulder
Edward Umheiser, DPT teaching the patient shoulder exercises.
Physical therapy along with treatment provided by your doctor such as cortisone injections are the first line of defense in reducing the time a patient may experience the symptoms related to a frozen shoulder.
A doctor will typically take some images of the shoulder to rule out other possible structural involvement such as the rotator cuff or the labrum.
At that point, physical therapy treatment 2-3x a week is generally recommended where manual shoulder stretching, massage, mobilization, and exercises are performed to keep the shoulder as pain-free as possible, and to help increase the range of motion.
It is also important to continue to perform the prescribed stretching exercises at home under the guidance of a physical therapist. Generally, the time it takes for a frozen shoulder to “thaw” can be halved under physical therapy treatment. Most patients do not need surgical intervention to correct this diagnosis.
Steps to Take If You Suspect Having a Frozen Shoulder
If you have noticed that you have a lot more difficulty with overhead shoulder motion following a shoulder injury, let your doctor know. If this has persisted for several months, it may be a sign of adhesive capsulitis. An orthopedist can help you make that diagnosis, and physical therapy can help you get onto the road to recovery.
Schedule Your Physical Therapy Appointment Today To Begin Frozen Shoulder Treatment
Physical Therapists play an essential role in the nonsurgical treatment of hip pain. Two of the most common conditions associated with hip pain are labral tears and hip impingement.
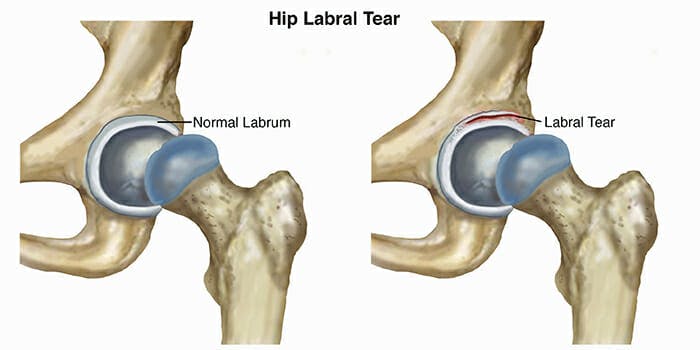
Labral Tears
Labral tears occur when the labrum, which is the cartilage that comes between the head of the femur – your thigh bone – and your pelvis – your hip bone, begins to wear down or experiences trauma. The most common cause of labral tears is repetitive stress on the hip joint, especially for athletes participating in running and skating sports.
Original Image Source: https://www.moveforwardpt.com/symptomsconditionsdetail.aspx?cid=fabdfb4e-5fb5-4077-b341-df5d04a93605
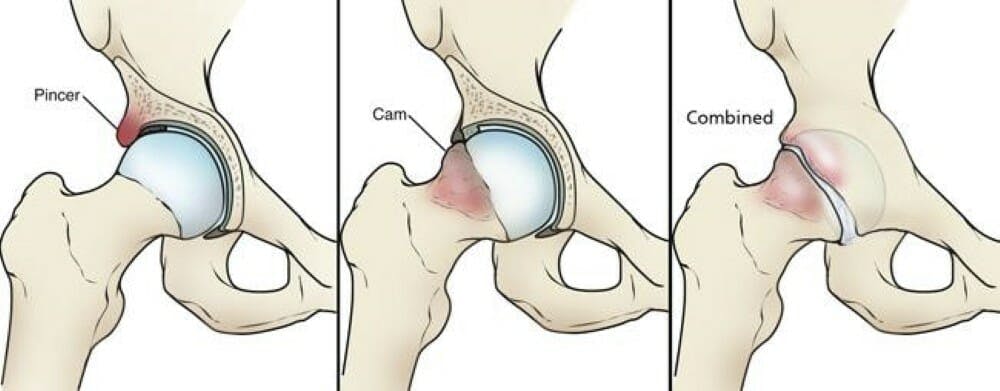
Hip Impingement
Hip impingement, also known as femoroacetabular impingement (FAI), occurs when extra bone grows on either or both the head of the femur or the acetabulum (the part of the pelvis where the femur meets – the “socket”). The extra bone creates an irregular fit and can start to rub against the cartilage or bones in a way that can damage the joint causing hip pain.
There are 2 types of hip impingement. They can occur separately or together.
Original image source: https://orthoinfo.aaos.org/en/diseases–conditions/femoroacetabular-impingement/
Cam-type Impingement
The head of the femur is shaped like a sphere. It acts as the “ball” for “ball and socket” joint in your the hips. In this deformity, an excessive bone growth around the head of the femur creates an irregular shape that makes it difficult to rotate in the acetabulum, your “socket”.
The misshapen overgrowth contacts the cartilage that lines the hip socket, the labrum, and can cause it to become worn and frayed. This can lead to hip instability and pain.
Pincer-type Impingement
Pincer impingement is when the acetabulum (hip socket) protrudes around the femur head, decreasing the space of the joint. Overtime with repetitive contact, hip flexion (bending over, sitting, walking) leads to tearing and inflammation of the cartilage that envelopes and protects the joint (labrum).
Symptoms
With either one of these conditions you may experience:
Increased pain with prolonged sitting and leaning forward in the sitting position.
Sharp pain during squatting, changing direction during running, pivoting and lateral motions./li>
Stiffness and deep aching in the front of the hip. Occasional groin pain.
Decrease ability to turn your thigh inward.
Treating Hip Pain with Physical Therapy
Treatment of hip pain starts with a comprehensive evaluation of movement of your hip and surrounding joints.
Our therapists will test the strength of the muscles around your hip and observe your movements to properly diagnose the condition. During each session, our therapists will instruct and educate you about your body mechanics, the origin of your injury, and exercises you can perform to prevent future injury to the hip and strengthen the muscles around the hip and other parts of your body to stabilize and correct any imbalances.
Your orthopedic doctor may order X-rays and an MRI to confirm the diagnosis.
Hip impingement and labral tears may be concurrent with lower back pain and pelvic floor dysfunction.
Once your weaknesses and imbalances are identified, the goal of therapy is to restore normal force coupling and to develop strategies to compensate if your condition is chronic.
Strengthening of weak muscles and stretching tight muscles can help to avoid the progression of hip impingement. Manual therapy techniques may also be employed restore flexibility of the joint.
At Park Sports Physical Therapy, one of our therapists, Svetlana Lazarev, PT, is an advance hip clinician certified by the Hospital for Special Surgery (HSS).
Hip Arthroscopy Post Operative Rehabilitation
If you do end up having surgery for your hip pain, our therapists follow an established post-surgical protocol. Physical therapy is known to shorten recovery time and ensures that your body is healing properly. Our therapists help to promote safe healing by limiting the weight you put on the operated leg, exercises, stretching, and manual therapy.
The next stage of postoperative rehabilitation focuses on improving your range of motion and strength. During your treatment, our physical therapists can keep your doctor and orthopedic surgeon informed of your progress if you choose.
After 4 to 6 months of treatment following surgery, you’ll be able to return to your normal activities.
Do you currently suffer from hip pain? We can help.
Sports injuries can occur from many different kinds of physical activities. This post will focus on how our occupational and physical therapists approach treating tendonitis, specifically for rock climbers feeling elbow, forearm, and finger pain.
Rock climbing is a very demanding sport requiring a lot of strength from your entire body. Grip strength is one of the most important factors in tackling new levels of difficulty in climbing. Working on strengthening your hands and forearms can prove to be challenging to develop without leading to injury.
Even professionals with many years of experience and skill can suffer from overworked flexors in their forearms and fingers.
When your flexors become inflamed from overuse – usually from your hands gripping tightly for prolonged periods of time – it can cause pain that can be felt from your fingers all the way to your elbow. This condition is called tendonitis.
So what do you do if you suffer from tendonitis? The first step is rest. For many athletes, this can be very difficult to do, especially if they are training for a competition. Some may even be tempted to continue to train, creating more inflammation and a bigger problem to deal with.
Exercises that require gripping should be avoided for a brief period time. Each case is very specific to the individual, so this will vary from person to person.
Simultaneously, to counteract the inflammation, direct application of ice or a cold pack to the affected area is recommended, especially if swelling is visible. After the inflammation has subsided, light stretching can be followed as tolerated.
To help with stretching, our certified hand therapists recommend using heat prior to stretching or exercise to allow the muscles and tendons to loosen up.
You can use a warm towel or heating pad to do this.
Below is one recommendation from one of our occupational therapists, Moussia Krinsky-Raskin, for stretching. Remember, you do not want to stretch to the point when you are feeling pain. There should be some discomfort, but never pain.
Straighten your arm in front of you as much as you can, bend your wrist towards your chest, palm facing you and hold for 5-10 seconds, or as much as you can handle it. This will stretch your extensors.
Straighten your arm in front of you, palm facing outward, gently pull the back of your hand towards your chest and hold for 5-10 seconds. This will stretch your flexors.
Recovering from tendonitis requires patience. Remember to listen to your body. Don’t ignore pain. Continue to push through the pain following the “no pain no gain” mantra can cause far more damage than good – regardless of mind over matter. A badly injured tendon rarely recovers to its full strength afterward. If pain continues for more than a few weeks, it is strongly advised that you see a medical professional.
Here are some tips on how you can prevent tendonitis in the future:
Take breaks often when training. Remember to treat rock climbing as if you were lifting heavy weights. There should be moments of rest between each “set” or climb that you attempt.
Stretch before and after training and rock climbing. It is important that you keep your muscles loose and mobile.
If you feel pain begin to creep up during your climb, stop. We understand that most people will disregard this piece of advice and want to continue training through the pain, but this will ensure longevity and maximum performance of your body in the long run. Don’t work yourself until you are out of commission!
Our physical therapists and occupational therapist are all sports rehabilitation specialists. They will work closely with you to help you recover quickly and teach you how to prevent injury in the future.
If you are just beginning to climb, we strongly encourage you to undergo a strength training program to help prep your body and prevent injury.
Do you currently suffer an injury from rock climbing? Our therapists can help.
Everyone has pelvic floor muscles. So why is it that almost all information relating to pelvic floor therapy focus solely on women?
There are obvious reasons why Pelvic Floor Therapy is normally associated with women’s health issues. For starters, Pelvic Floor Dysfunction is far more prevalent in women than men, especially pregnant women.
Although this is true, there is still a fair amount of men suffering from symptoms associated with pelvic floor dysfunction. What’s worse is that most of them don’t even know it.
In fact, many times even medical doctors can misdiagnose pelvic floor dysfunction with much more serious conditions and diseases since symptoms can feel very similar to them. Sometimes this can lead to prescribing unnecessary medications and antibiotics, and in more extreme cases, surgery.
All of this could be preventable if men were more informed about their bodies and if medical practitioners knew more about pelvic floor issues.
When men suffer from erectile dysfunction, painful urination, frequent & involuntary urination, painful ejaculation, constipation, or pain after having a bowel movement, the last thing they would suspect is a problem with their pelvic floor muscles. And who can blame them?
Pelvic Floor Therapy for Men
At Park Sports Physical Therapy, part of our mission is to educate our patients about their bodies and the reasons they feel the symptoms that they do. We also stress the importance of preventative care, and the steps they can take through exercise and posture to keep them functional.
Our pelvic floor specialist, Irene Hernandez, DPT, specializes in treating both women AND men. We strongly encourage our male patients suffering from any of the conditions or symptoms listed above to come in for an evaluation.
The pelvic floor plays a few roles. For one, it is a group of muscles that form the “bottom” of your body’s core. This keeps the organs in place and from dropping out of the pelvis.
The second major responsibility of the pelvic floor is the control of the sphincters. This includes the anus and urethra. Weak pelvic floor muscles can result in incontinence – or the inability to hold in urine and/or feces. An over contracted pelvic floor will make it difficult to make a bowel movement, leading to constipation, or the inability to release urine.
The third major responsibility of the pelvic floor is sexual function. For men, dysfunction of the pelvic floor can lead to erectile dysfunction (ED). There are many other factors that can play into ED, but seeing a pelvic floor specialist can alleviate and correct muscles related to healthy sexual function.
Male Pelvic Floor Medical Illustration – Illustrated by Amy Stein – Heal Pelvic Pain Original Source: https://www.healpelvicpain.com/
If you’re a fan of baseball you may have heard that New Los Angeles Angels pitcher, Shohei Ohtani, has a damaged Ulnar Collateral Ligament (UCL) in his pitching arm.
This is bad news for Ohtani, as his career relies heavily on the function his elbow. Although reports show that Ohtani only has a first-degree sprain, consistent use of his elbow can present serious problems down the line.
In the world of physical therapy, elbow pain does not get enough exposure and is often ignored. More often than not, people continue performing their daily activities that can exacerbate injury to the elbow and cause damage to the joint and ligaments.
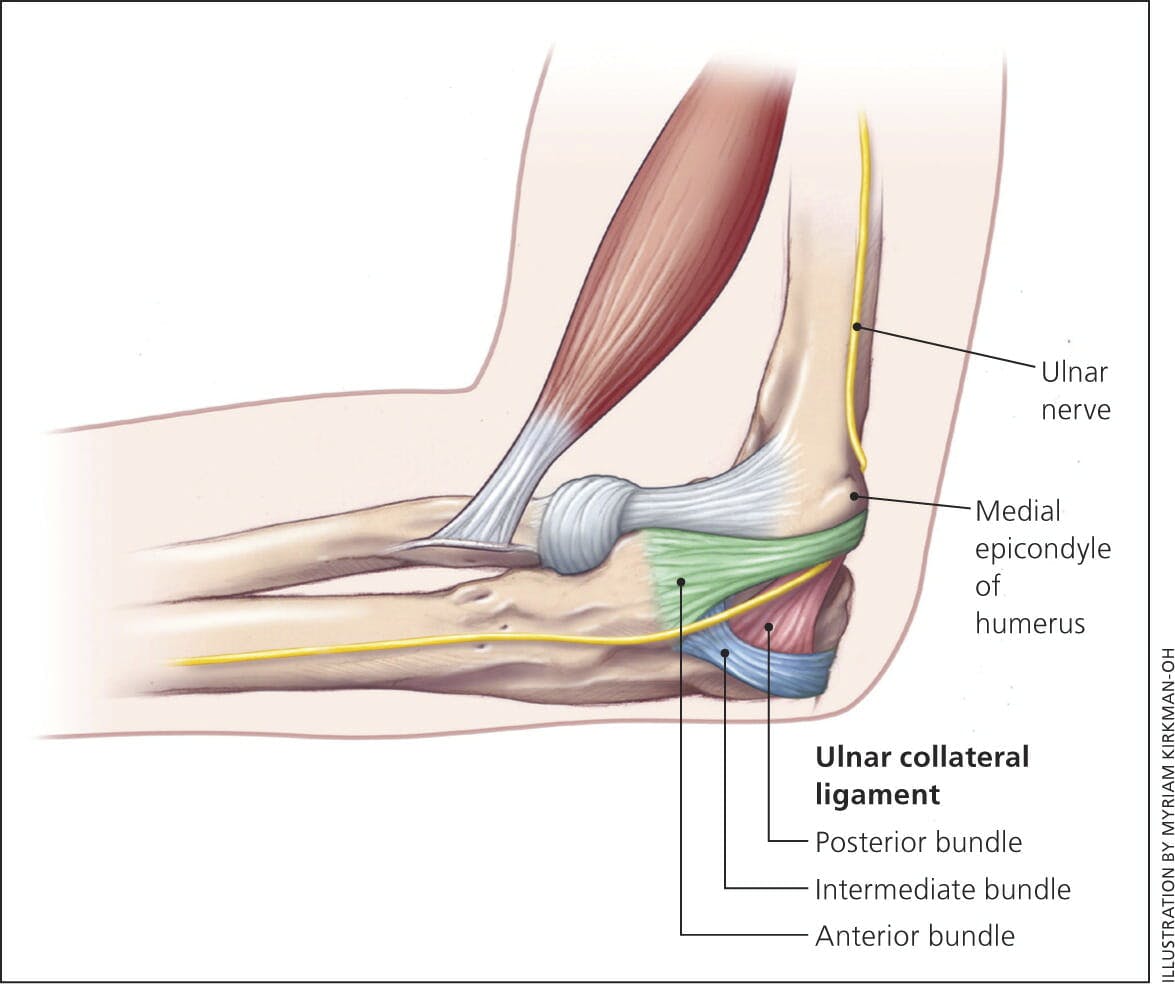
Ulnar Collateral Ligament (UCL) Injury
As Physical Therapists, we see sports injuries in a different light, especially when they make the news. This post will share some of the intimate knowledge we possess from years of treating a number of injuries and conditions that athletes may face.
The Ulnar Collateral Ligament, located in the elbow, is a complex structure consisting of three bands. It is challenged more when the elbow is in flexion. During full elbow extension, the bony congruity provides additional stability.
Ulnar Collateral Ligament injury is common in many overhead sports. The forces that can lead to injury on the elbow are generated when the elbow goes from flexion to extension at a high velocity. In Ohtani’s case, this would be frequently pitching at a consistent speed of 100 mph.
This injury occurs from repetitive valgus (a condition in which the bone segment distal to a joint is angled outward) stress on the medial (inner aspect) of the elbow. This kind of elbow sprain commonly occurs in baseball pitchers. It is less frequent in racket sports, volleyball, and hockey, but can still occur in athletes playing those sports.
Damage to the ligament can be caused by sudden trauma or a gradual stress. The most typical sign is a pain in the inner elbow while performing a physical activity. Patients commonly describe an elbow sprain as a twinge or sharp pain when pushing up, such as getting up from the chair.
If a ligament is compromised a patient may develop:
A sense of looseness or instability in the elbow.
Irritation of the ulnar nerve (aka the “funny bone”): This is felt as a tingling sensation or numbness in the small finger and ring finger.
Decreased ability to throw a baseball or other object overhead.
Treatment for Ulnar Collateral Ligament Injury
Ulnar Collateral Ligament injury can happen to anyone at any age. Parents and coaches should be aware of the issue and be alert if the child complains of the pain in the elbow.
Physical Therapy is the best first line of defense following this diagnosis. At Park Sports Physical Therapy, our Physical Therapists are skilled and experienced in treating elbow instability and ulnar collateral ligaments tears.
The treatment approach is based on thorough examination and biomechanical analysis of the activity that caused the condition.
It includes:
Strengthening weak muscle group
Activity modification.
Manual therapy and therapeutic modalities.
Post-Surgical Recovery
In cases of severe damage and instability, the ligament is reconstructed in what is commonly known as a Tommy Johns procedure. Physical Therapy treatment in this case follows an established post-surgical protocol. Our therapists work closely with an Orthopedic Surgeon to optimize post-surgical recovery and achieving the highest functional outcomes.
Do you suffer from Ulnar Collateral Ligament Injury? Take the first step to get out of pain by scheduling your appointment.
Scoliosis affects 2-3% of the American population. The most common form being idiopathic scoliosis which affects children ranging from ages 10-15 years old. Idiopathic means the causes are unknown. It is typically detected by school screenings or a physician visit. Patients with idiopathic scoliosis rarely experience pain and the curve is usually minor enough that treatment isn’t needed, but this can change with time. If your child has scoliosis our certified Schroth therapists can help treat and teach your child how to counteract the imbalances caused from the abnormal curvature of the spine.
In this article, Park Sports founder and physical therapist Boris Gilzon, PT DPT, OCS, CHT describes how our therapists utilize conservative methods such as breathing techniques, exercise, and body awareness to address Scoliosis and Kyphosis.
Originally developed in Germany by Katharina Schroth in the early 1920’s, the Schroth method has become one of the most effective and safest approaches to treating Scoliosis.
The Schroth method focuses heavily on rotational breathing, stabilizing and balancing the spine, chest expansion, derotation and reduction of the spine’s irregular curvature, elongation of the spine, hands-on treatment to correct the body’s posture, and educating the patient on exercises and techniques they could use for life.
There are numerous Schroth Method exercise. The combination of exercises our physical therapists prescribe is based on each patient’s body and the curves of their spine.
Unlike most other exercises, which are completed on both sides of the body, scoliosis exercises are generally executed on one side only. This is in order to correct the imbalances of the spine by lengthening and strengthening the muscles in this area.
On the whole, the exercises consist of a combination of stretching, strengthening and breathing techniques, which follow this three-step exercise process:
First, make sure the pelvis is properly aligned
Then, do exercises to lengthen the spine, followed by breathing techniques to move the spine and ribs into the best possible posture
Finally, tense the muscles of the trunk, which will strengthen weak muscles and preserve the posture that has now been corrected
The benefits of the Schroth Method are highlighted in the findings of this recent study:
According to these results, Schroth PSSE (physiotherapeutic scoliosis-specific exercises) added to the standard of care were superior compared to standard of care alone for reducing the curve severity in patients with AIS (adolescent idiopathic scoliosis).Reference: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5198985/
So if you or your child are dealing with scoliosis, the Schroth Method may be your best option to address its symptoms and prevent the condition from progressing further.
Do you or your child suffer from scoliosis or kyphosis? We can help. Schedule your evaluation today.
.png?auto=format&auto=compress&h=150)